Important Vocab Terms
- Cardiac Output (CO): The amount of blood pumped by the heart per minute.
- Formula: CO = Heart Rate × Stroke Volume
- Normal: 4-8 L/min
- Stroke Volume (SV): Amount of blood ejected from the left ventricle with each contraction.
- Ejection Fraction (EF): Percentage of blood pumped out of the left ventricle with each beat.
- Normal: 55-70%
- Preload: The amount of blood returning to the heart. Excessive preload can cause fluid retention, congestion in the lungs, and increased workload on the heart.
- Afterload: Resistance the left ventricle must overcome to eject blood. Increased in hypertension.
- Mean Arterial Pressure (MAP): Average arterial pressure during one cardiac cycle.
- Goal: ≥ 65 mmHg for adequate organ perfusion.
- Systole: Ventricular contraction phase.
- Diastole: Ventricular relaxation and filling phase.
- Myocardial Infarction (MI): Necrosis of heart muscle due to prolonged ischemia.
- Angina: Chest pain caused by myocardial ischemia.
- Heart Failure (HF): Inability of the heart to pump sufficient blood to meet body demands.
- Atrial Fibrillation (AFib): Irregular atrial rhythm that increases stroke risk.
- Cardiogenic Shock: Pump failure leading to decreased tissue perfusion.
- Troponin: Cardiac enzyme elevated with myocardial injury.
- BNP (B-type Natriuretic Peptide): Elevated in heart failure.
Cardiac Electrical Conduction System
The order in which an electrical impulse travels to create a heartbeat:
- SA Node → AV Node → Bundle of His → Right & Left Bundle Branches → Purkinje Fibers
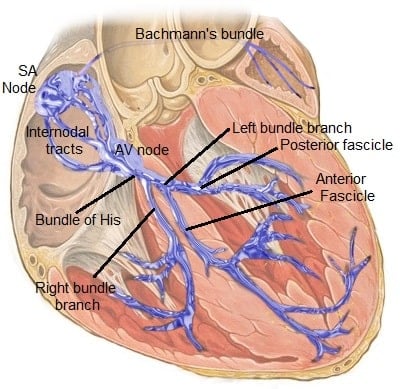
Figure A: Image providing an overview of the cardiac electrical conduction system.
You should be aware of the following:
- Normal Heart Rate: 60-100 bpm
- Bradycardia: <60 bpm
- Tachycardia: >100 bpm
Here is a summary of what intervention is most appropriate for specific cardiac rhythms you may see on the NCLEX:
| Rhythm | Pulse? | Treatment |
| Symptomatic Bradycardia | Yes | Atropine |
| Ventricular Tachycardia | Yes | Cardioversion |
| Ventricular Tachycardia | No | Defibrillation + CPR |
| Ventricular Fibrillation | No | Defibrillation + CPR |
| Asystole | No | CPR + Epinephrine |
Coronary Artery Disease (CAD) & Myocardial Infarction (MI)
Here is a table summarizing CAD & MI:
| Condition | Description | Key Features | High-Yield NCLEX Point |
| Stable Angina | Predictable chest pain caused by temporary myocardial ischemia during exertion or stress. Relieved by rest or nitroglycerin. No permanent heart damage. |
– Predictable pattern – Triggered by exertion or stress – Relieved by rest or nitroglycerin – No myocardial cell death |
|
| Unstable Angina | Unpredictable chest pain due to reduced coronary blood flow, often occurring at rest. Not reliably relieved by rest. Medical emergency. |
– Occurs at rest – Increasing severity or frequency – Not consistently relieved by rest – No myocardial cell death |
|
| NSTEMI (Non-ST-Elevation Myocardial Infarction) | Myocardial infarction caused by partial coronary occlusion resulting in myocardial cell death without ST elevation on ECG. |
– Elevated troponin – No ST elevation – Partial coronary blockage |
|
| STEMI (ST-Elevation Myocardial Infarction) | Severe myocardial infarction caused by complete coronary occlusion producing ST elevation on ECG and requiring immediate reperfusion. |
– ST elevation on ECG – Elevated troponin – Complete coronary blockage – Immediate treatment required |
|
| Myocardial Infarction (General) | Heart muscle injury caused by blocked coronary blood flow. |
– Chest pressure or heaviness – Radiating pain to arm or jaw – Diaphoresis – Nausea – Shortness of breath |
– Chest pressure + diaphoresis + nausea = suspect MI |
| Silent Myocardial Infarction | Myocardial infarction with minimal or atypical symptoms, more common in diabetics and women. |
– Fatigue – Dyspnea – Indigestion-like discomfort – Little or no chest pain |
– Diabetic patient + unexplained fatigue or dyspnea = consider silent MI |
Emergency Management
MONA
MONA is a traditional mnemonic for early myocardial infarction management.
- Morphine: Reduces pain and anxiety; decreases preload and myocardial oxygen demand.
- Oxygen: Given if hypoxic (SpO₂ < 90%) to improve oxygenation.
- Nitroglycerin: Vasodilates coronary arteries. Reduces chest pain and preload.
- Aspirin: Antiplatelet. Prevents further clot formation.
Priority: Aspirin first, unless contraindicated (e.g., allergy, active bleeding). It reduces mortality by limiting clot expansion.
Other Key Treatments
- Beta blockers: Decrease heart rate, blood pressure, and myocardial oxygen demand.
- Anticoagulants: Prevent further clot propagation (heparin).
- PCI (Percutaneous Coronary Intervention): Angioplasty with stent placement to restore blood flow. Preferred treatment for STEMI.
- Thrombolytics: Clot-busting medications used if PCI is not immediately available.
Major Complications After MI
- Dysrhythmias: Abnormal heart rhythms caused by faulty electrical impulses.
- Cardiogenic Shock: Severe pump failure leading to hypotension and poor perfusion.
- Heart Failure: Reduced cardiac output due to damaged myocardium.
Heart Failure
Left-Side Heart Failure
Failure of the left ventricle causes blood to back up into the lungs, leading to pulmonary congestion.
Symptoms:
- Crackles
- Dyspnea
- Orthopnea
- Pink frothy sputum
- S3 heart sound
Right-Side Heart Failure
Failure of the right ventricle causes blood to back up into systemic circulation, leading to peripheral fluid overload.
Symptoms:
- Peripheral edema
- Jugular venous distention (JVD)
- Hepatomegaly
- Weight gain
Systolic vs. Diastolic Heart Failure
Systolic HF (HFrEF): Reduced ejection fraction (< 40%) due to impaired ventricular contraction.
Diastolic HF (HFpEF): Normal ejection fraction but stiff ventricle causes impaired filling during diastole.
- Systolic = pumping problem
- Diastolic = filling problem
Hypertension
Hypertension is a chronic elevation in blood pressure that increases strain on the heart and blood vessels, leading to long-term organ damage.
Blood Pressure Categories
- Normal: <120 systolic / <80 diastolic
- Elevated: 120-129 systolic / <80 diastolic
- Stage 1: 130-139 systolic or 80-89 diastolic
- Stage 2: ≥140 systolic or ≥90 diastolic
Major Complications
Chronic high pressure damages blood vessels and target organs:
- Stroke: Vessel rupture or clot formation in the brain
- Myocardial Infarction (MI): Increased cardiac workload and coronary damage
- Kidney Failure: Damage to renal blood vessels
- Retinopathy: Vision changes due to retinal vessel damage
Hypertensive Crisis
Severely elevated blood pressure:
- Systolic >180 and/or Diastolic >120
This can lead to acute organ damage. Symptoms of organ involvement include:
- Severe headache
- Vision changes
- Chest pain
- Neurologic deficits (confusion, weakness)
Hypertensive Emergency vs Hypertensive Urgency: The parameters remain the same but Hypertensive Emergency has signs of acute target organ damage while Hypertensive Urgency does not have acute target organ damage. IV meds are used in emergency while urgency is usually treated with oral medications.
Priority Treatments
- IV antihypertensives (e.g., labetalol, nicardipine)
- Continuous blood pressure monitoring
Dysrhythmias
Dysrhythmias (arrhythmias) are abnormalities in heart rate or rhythm that can reduce cardiac output and lead to hemodynamic instability.
| Condition | Description | Key Findings | Treatment |
| Atrial Fibrillation (AFib) | A chaotic atrial rhythm causing ineffective atrial contraction and an irregular ventricular response. |
– Irregularly irregular rhythm – No distinct P waves – Variable ventricular rate |
– Rate control (beta blockers, calcium channel blockers) – Anticoagulation to prevent embolic stroke |
| Ventricular Fibrillation (VF) | Chaotic ventricular rhythm with no effective contraction. Medical emergency. |
– No cardiac output – No pulse |
– Immediate defibrillation – CPR |
| Asystole | Complete absence of electrical activity (“flatline”). |
– No electrical rhythm – No pulse |
– CPR + Epinephrine – Do NOT defibrillate |
High-Yield Cardiac Medications
Here is a table of some important cardiac medications you should be familiar with:
| Medication Class | What It Does | Example | Key Nursing Consideration |
| ACE Inhibitors | Block conversion of angiotensin I to II, lowering blood pressure and reducing cardiac workload. | Lisinopril | Monitor potassium, watch for cough |
| Beta Blockers | Decrease heart rate and blood pressure by blocking beta-adrenergic receptors. | Metoprolol | Hold if HR < 60 |
| Calcium Channel Blockers | Relax vascular smooth muscle and decrease heart contractility to lower blood pressure. | Diltiazem | Monitor BP |
| Loop Diuretics | Promote rapid excretion of sodium and water to reduce fluid overload. | Furosemide | Monitor potassium |
| Nitroglycerin | Vasodilates coronary arteries to improve myocardial oxygen supply. | SL Nitro | Check BP before giving |
| Digoxin | Increases cardiac contractility and slows heart rate. | Digoxin | Hold if HR < 60, monitor potassium |
| Anticoagulants | Prevent formation and extension of blood clots. | Heparin, Warfarin | Monitor bleeding, labs |
| Thrombolytics | Dissolve existing blood clots to restore perfusion. | Alteplase | Risk of hemorrhage |
Cardiac Labs & Priority Assessment Findings
Here are some cardiac lab items you should be familiar with:
- Troponin: Elevated with MI
- BNP: Elevated in heart failure
- CK-MB: Cardiac enzyme
- ECG: Detects ischemia and dysrhythmias
- Echocardiogram: Measures EF
- Cardiac Catheterization: Identifies blockages
Here are the most concerning assessment findings:
- New chest pain
- ST elevation
- Severe hypotension
- Oxygen saturation <90%
- Decreased urine output
- Altered mental status
Image Source: “Cardiac Conduction System“, by Npatchett [CC BY 4.0]